Based on Current Reviews and Meta-analyses We Can Say That Cybertherapy Generally Appears to Work
![]() Open up access peer-reviewed chapter
Open up access peer-reviewed chapter
Virtual and Augmented Reality: New Frontiers for Clinical Psychology
Submitted: October 16th, 2017 Reviewed: January 24th, 2018 Published: May 23rd, 2018
DOI: 10.5772/intechopen.74344

IntechOpen Downloads
two,290
Total Chapter Downloads on intechopen.com
![]()
Altmetric score
Overall attention for this chapters
Abstruse
In the concluding decades, the applied arroyo for the utilize of virtual reality (VR) and augmented reality (AR) on clinical and wellness psychology has grown exponentially. These technologies take been used to treat several mental disorders, for instance, phobias, stress-related disorders, low, eating disorders, and chronic pain. The importance of VR/AR for the mental health field comes from three main concepts: (1) VR/AR as an imaginal technology, people tin feel "as if they are" in a reality that does not exist in external earth; (2) VR/AR equally an embodied technology, the feel to feel user'southward body inside the virtual environment; and (3) VR/AR as connectivity technology, the "finish of geography'. In this chapter, we explore the opportunities provided past VR/AR as technologies to improve people's quality of life and to discuss new frontiers for their application in mental wellness and psychological well-beingness promotion.
Keywords
- virtual reality
- augmented reality
- cybertherapy
- clinical psychology
- advantaged technology
*Accost all correspondence to: saven2@alumni.uv.es
1. Introduction
Clinical psychology is generally perceived equally a face-to-face interaction between therapist and patient. However, thanks to technology developments, this picture has been changed. The massive innovation of Information and Communication Technologies (ICTs) has brought a revolution to the view of psychology and likewise the way how psychotherapists work [1]. Especially, the application of virtual reality (VR) and augmented reality (AR) has given an important contribution to mental health.
In the last decades, a growing number of studies have shown of import implications of the use of ICTs for treating several disorders and promotion of well-being. Initially, about of these studies take focused on treating anxiety disorders [2], phobias (e.yard., specific phobias, social phobia, agoraphobia) [3], posttraumatic stress disorder (PTSD) [4, 5], eating disorder [6], habit to nicotine or alcohol [seven, 8], among others. Furthermore, VR and AR have been used not only for clinical intervention just also for promoting good for you lifestyles or well-being, for example, the reduction in stress [nine], handling of pain in oncology patients [ten], or pain management for variety of known painful medical procedures [11]. In all these studies, the utilize of these ICTs has supported psychotherapists and researchers to reach the all-time results for patients. Cheers to the technological advances, information technology is possible to reproduce virtual surround where people tin motility as they are in the existent globe [12], or having some mobile applications which can overstate the world around united states of america and facing specific phobia [thirteen]. But for professionals, it is not always an easy work because the utilise of ICTs usually implies that psychologists accept to open their mind and co-piece of work with engineers and other professionals who have different backgrounds. Psychologists and engineers have to discover a way to cooperate and to integrate their knowledge, a cooperation that till now has changed society exponentially.
In this chapter, nosotros review some of the most important advances in this field and how technology can (or could in the time to come) support clinical psychology. The aim is to explore the opportunities provided past VR and AR every bit technologies to improve people's quality of life and to talk over new frontiers for their application in mental health and psychological well-existence promotion.
Advertisement
2. What is cybertherapy?
Cybertherapy is the branch of psychology that uses ICTs to induce clinical change [1]. It is also divers as the employ of advanced technologies, such as virtual or augmented reality, equally an offshoot to traditional form of therapy. Cybertherapy is rapidly condign an accustomed and validated method for the treatment of many unlike wellness care concerns. Information technology occurs considering engineering science supporting "cybertherapy" provides visual and auditory stimulus that may be otherwise difficult to generate, and it can back up and motivate operation, as in rehabilitative exercises [14]. Also, other ICTs are becoming increasingly mutual in clinical psychology. It is generally like-minded that innovative e-therapy approach is an opportunity for earlier and better treat the virtually mutual mental health problems. E-therapy approach allows the patient to engage in treatment without having to conform the function appointment, oft reducing other limitations in face-to-face up treatment [15].
These advances come up from the role of telemedicine and e-wellness. Telemedicine has been defined as the employ of telecommunication technologies to provide medical information and services. The defining aspect of telemedicine is the employ of electronic signals to transfer information from ane site to another. Information technology can be useful for situations in which physical barriers prevent the set up transfer of data between patients and wellness care providers, and the availability of data is the central to proper medical management [16].
Since 1988, Norwegian Telecom Research has initiated and developed several telemedicine applications; the applications were adopted to exchange medical results from clinical chemistry to interactive radiology consultations. All the applications have a common goal to improve efficiency and quality of wellness care. One of the basic ideas of telemedicine tin can be expressed by the maxim: "Movement the information, not the patient" [17]. Indeed, i of the starting time telemedicine programs was proposed by rural practitioners who required access to sure type of medical services [17].
According to Eysenbach, e-health interventions are defined as treatments, typically behaviorally based, that are operationalized and transformed for delivery via the Internet [18]. A branch of e-health is eastward-mental health, or Net-based therapy, in which electronic equipment and therapeutic communication converge. E-mental health can be defined as using ICTs to put patients and mental health professionals in contact; to conduct diagnosis or treatment; to disseminate data; or to acquit enquiry studies or any other activity related to mental health care [xix]. The online services include email, discussion lists, chats, or audiovisual conferencing, but likewise computerized treatments.
The principal advance of online therapy is that it can reach people who might not otherwise seek therapy, such as disabled people or those who live in remote areas; information technology also reduces the contact time between therapist and patient [20]. Today, it is possible to make counseling through Internet, avoiding the face-to-face communication. It does not mean that man interaction disappears, and on the contrary, it faces relevant obstacles such as geographical distance, timetable, and emotive aspects that prevent patients to seek for a psychological therapy [17].
Mohr and colleagues [21] brought the e-wellness to a forrard step. Mohr underlines the "behavioral intervention technologies" where technologies, such equally telephone, videoconferencing, and web-based interventions, are integrated with other advanced technologies such equally sensors for monitoring, social media, VR, and gaming, promoting due east-mental-health interventions. From this perspective, e-mental-health not only provides new delivery media for mental health treatments, but opens the possibility for entirely new interventions. For example, mobile technologies can harness sensors and ubiquitous calculating to provide continuous monitoring and/or intervention in the patient'southward environment. VR creates simulated environments that afford a high degree of command in engineering the provision of therapeutic experiences. Gaming may provide teaching methods that are more engaging. These opportunities may likewise claiming and expand the limits of the knowledge regarding homo beliefs processes [18].
Afterwards this overview, we tin consider cybertherapy as a ramification of e-mental health. It includes all those kinds of treatment done through interactive and immersive technologies such as virtual and augmented reality where people become involved in the "digital" environments. As mentioned, cybertherapy has been used to care for psychological conditions such as anxiety disorders and phobias, eating disorders, autism, substance abuse and addiction, to reduce pain and discomfort perceived during unpleasant medical treatments, to manage stress, to administer exercises for cognitive rehabilitation (eastward.chiliad., memory and attention disorder), and so on [22]. Evidence has shown that cybertherapy outcomes are comparable with those obtained through therapy protocols that are not supported past technologies [23], with some boosted advantages that may make cybertherapy a preferable choice. The most obvious advance is that the mediated environment allows patients to feel situations, to display stimuli, or to provide feedback of the patient's activeness that in vivo would be not controllable (e.g., crowd behavior), non feasible (east.g., scenario variation to improve transfer of skills), or unavailable (e.g., an iced world mitigating pain during medical treatment from severe burning) [22]. In addition, the use of mediated surround minimizes implementation failures because a mediated environs embeds the administration transmission: standard task educational activity and explanations, organizations of stimuli into subsequence treatment steps, and setting options for personalized handling. As Botella and colleagues have pointed out [22], the use of ICTs in delivering a psychological therapy allows handling to reach people in critical conditions, to improve persistency, ubiquity, anonymity, and multimodality of an intervention, too equally the ease with which data can be stored, accessed, and manipulated.
Cybertherapy can adopt dissimilar formats: from totally self-guided to more than blended, including the presence of the therapist in different graduations, and the protocol tin as well include other treatments in add-on to the virtual one [24].
In technical terms, hardware and software are combined into cybertherapy to accomplish the last therapeutic goals. The software content embeds and makes concrete abstract scenarios, imagined situations, feared objects, subjective symbols, and meaning. The hardware shapes the way in which those contests are experienced, whether in isolation from the surrounding or merged with them and whether involving the body in a natural interaction with the environment or mediating the interaction with input devices [25].
Every bit we said earlier, cybertherapy includes dissimilar types of technologies. Now, we focus on two of them: VR and AR.
2.1. Virtual reality in cybertherapy
VR is a collection of technologies that allow people to interact efficiently with 3D computerized database in real time using their natural sense and skills [26]. In terms of behavioral science, VR has been described equally an advanced class of human-computer interface that allows the user to interact with and become immersed in a computer-generated environment in a naturalistic manner [26]. VR has emerged every bit a potentially effective way to provide general and specialty health care services and appears poised to enter mainstream psychotherapy delivery.
Where does the utilise of VR in cyberpsychology come from? The pioneering work past Watson demonstrated, contrary to the dominant Freudian theories of psychology, that it was possible to stimulate phobias in a laboratory environment. The petty Albert experiment provided empirical evidence of classical conditioning in human. Few years later a study was conducted with the patient named Peter [27]. The therapist treated his rabbit phobia with classical status model: a pleasant stimulus (food) was presented simultaneously with the rabbit. This case illustrated how fearfulness may be eliminated under laboratory weather condition. The written report was a pioneer which introduced evidence-based psychological procedures to the field of psychological treatment through the application of "exposure therapy" [22].
The rationale behind VR employ to help exposure technique is simple: in VR, the patient tin can be intentionally confronted with the feared stimuli while allowing the anxiety to attenuate. What distinguishes VR from other media or communication systems is the sense of presence. What is "presence"? Generally, the sense of presence has been defined equally a mental state in which a user feels that he/she is beingness there, in the calculator-mediated surround [28]. These characteristics of VR offer a number of advantages, as we explain below, over in vivo or imaginal exposure [26].
Since the early 1990s, when Hodges and colleagues [26] reported that the use of virtual environment can provide to acrophobic patients the feeling of heights in a prophylactic situation, VR exposure therapy has been proposed as a new medium for exposure therapy [29]. In the past decade, numerous studies have tested the efficacy of VR. Review and meta-analysis [30] studies show how VR therapy works more finer than imaginal therapy (visualization) and equally finer as in vivo exposure therapy [31].
To give a clearer idea about the intervention trough VR, we explicate beneath the intervention for people with flying phobia fabricated by Botella and colleagues [32]. The program includes three virtual scenarios: (i) living room: here, the participant can perform some activities usually associated with the days or hours before the flying: pack, listen the TV news almost the weather, and accept his/her ticket for the bank check-in; (2) drome: the fourth dimension before flight is simulated. The participant tin heed and come across on the monitor for the announcement of boarding pass, knowing that his flight is near, and mind to other people talking about the flights. It is as well possible to encounter and hear planes landing and accept-off. At the end, participant can enter into the virtual airplane scenario; (3) airplane: the participant is sitting on the airplane and can feel take-off, flight, and landing in different conditions (turbulences, storm, etc.) Through the previous virtual environment description, it is possible to figure out how much VR reflects the reality.
VR offers several advantages as new options to patients who are unable to utilize imaginal therapy due to difficulties engaging with a situation, or who are resistant to in vivo handling due to farthermost anxiety. It is recognized that there is a big percentage of population (over 80%) that cannot visualize effectively. In addition, many of those suffering from feet practise not feel that they tin can arroyo their feared state of affairs in real life [22].
In add-on, VR has an advantage to create safe virtual globe where the patient can explore and experience "new realities"; this feeling of condom is essential in therapy, and so that the patient tin can act without feeling threatened. Moreover, in VR, data can exist presented gradually, in such a way that the patient can progress from easier tasks to more than hard one. This work in the virtual earth helps patients master the strategies need to overcome their fears and limitations in the existent world. Furthermore, equally VR goes beyond space and fourth dimension, researchers do not take to expect for specific events to occur. Rather, they can simulate them whenever appropriate for the patient and the therapy process [26].
In summary, VR protocols tin offer to clinicians and researchers a practical tool to back up the clinical tasks (cess and treatment) in ecologically valid, safe, and controllable environments [33].
ii.2. Augmented reality in cybertherapy
AR is a modification of VR which includes a combination of both real and virtual elements. The most significance aspect of AR is that the virtual elements add relevant and helpful input to physical information available in the real world. User can see images that blend both "real-globe elements" and "virtual elements" that take been introduced by the system [13].
As is explained in Table ane, in that location are differences between AR and VR. The commencement departure is the immersion of the user within the organization. VR achieves an involved environment for the user and perceptive channels such as vision and sound are controlled by the system. Contrarily, the AR arrangement complements the real world being necessary that the user maintains his/her sense of presence in that world. AR has a mechanism that combines the real and the virtual scenes that is not present in VR settings. In the AR system, the virtual objects generated by computer must exist completely fused to the real world, in all of the dimensions.
| Area | Virtual reality | Augmented reality |
|---|---|---|
| Immersion | User is completely immersed into the virtual environment | User can see their own body in context |
| Indicate of view | Egocentric and allocentric | Allocentric |
| Sense of presence | Feel inside the virtual world | Go on feeling inside the "real" world |
| Environment | Substitutes the existing environment with the virtual one | Uses virtual elements to build upon the existing surround |
| User experience | Generates new experience | Enhancing the experience |
| Time study | Since the beginning of twentieth century | Since the last few years |
| Toll | Higher | Lower |
Tabular array 1.
Principal departure between VR and AR in clinical psychology.
In few words, while VR immerses fully the user in the entire virtual surroundings, AR permits the user to run into the existent world, with the important departure that virtual object merges with bodily ones in a blended epitome [34]. Co-ordinate to Milgram and Kishino [35], AR is a course of mixed reality, that is, a particular subclass of VR-related technologies that, via a single display, expose the user to electronically merged virtual and nonvirtual elements.
AR has been used in various fields such as education and teaching [36], medicine and surgery [37]. Nonetheless, AR applications for psychological treatment are still deficient and address mailing phobias [33]. Preliminary data evidence the utility of the system for the treatment of insect phobia [thirteen]. Below is described a report for cockroach phobia to underline how AR system works in therapy (Figure ane) [13].
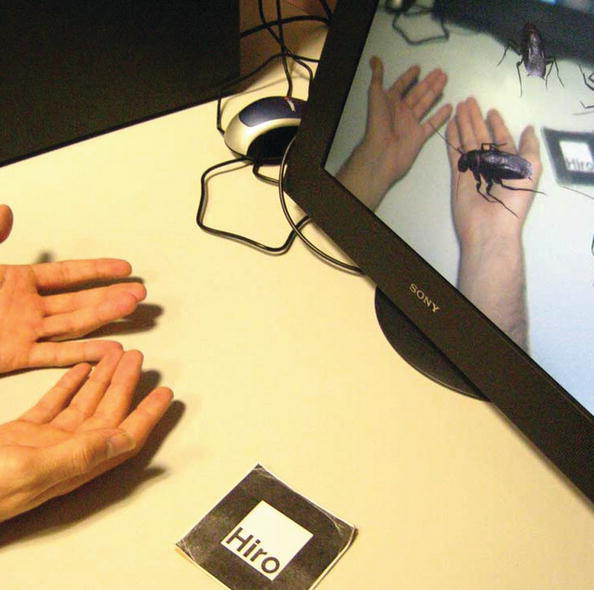
Figure 1.
Cockroach AR system.
AR-cockroaches system was adult using a proper engineer software. Information technology uses computer vision techniques in order to obtain the position and orientation of the photographic camera with respect to markers. When the photographic camera found a mark in the existent world, the program recognized it and activated the feared virtual surroundings (cockroach). The virtual insect that nigh appears in the easily of participants (cockroach in this example) looks real thanks to a peculiar AR technology. The therapist can picket the virtual stimuli presented to participants during the exposure session in the monitor and tin command the application using computer keys (number of cockroaches, motion, size, etc.). All of these combined cockroach'due south options enable the therapists to apply the treatment progressively [xiii]. This attribute put focus on the main advantages of AR as information technology was figured out also in VR: the feeling of safety [22]. In AR, it is possible to modify the virtual elements through the participant consent which reduces their rejection for therapy.
AR offers boosted advantages: it can provoke not bad feeling of presence because the environments and the tools with which the participants interact are real. In AR, the users can encounter their own body in the surround and interact with the fearing stimuli; in addition, the system allows patients to use existent elements and their ain hands and body to interact with stimuli.
These pioneer studies show that AR can be a very important culling treatment for phobia and might exist useful for other psychological disorders.
Advertisement
3. The central concepts of virtual and augmented reality for clinical psychology
The artificial environment generates from virtual and augmented reality is closer to daily life people. That is why virtual environment can be considered as an "ecological laboratory" where behaviors, feelings, and human being experience can be studied in a controlled and rigorous way [38].
Virtual and augmented reality can ameliorate some aspects of available treatments [33]. Equally mentioned, the ecological validity of the assessment could be even better than "in vivo" therapy. First, with AR and VR, the therapist has full control over the virtual situations and elements in the computer program, such as the generation of stimuli, including their club of advent and their quantity. 2nd, they tin can brand patients feel more than secure during therapy considering outcomes that they fear will happen in the real globe cannot happen in AR and VR (without consent and planning). For case, the therapist can expose a patient to a virtual elevator and assure him/her that it will non break down, or tin expose a patient to a flight with no turbulence. As the patient progresses, the therapist can program more hard exposure tasks. Third, AR and VR enable easier admission to threatening stimuli. This efficacy is significance considering information technology is non ever easy to obtain real elements such as cockroaches or spiders as needed for therapy [22]. In other works, it could be assumed that VR and AR tin have numerous applications in the field of psychological treatments. Co-ordinate to Riva [26], these advantages position VR equally an "intermediate pace between the therapist'south office and the existent earth."
We focus the hereafter perspective of VR and AR on three main aspects which contribute to increase their efficacy and affectivity in clinical psychology. Equally we described below, VR and AR could be considered as imaginal applied science, embodied applied science, and connectedness technology.
iii.1. Imaginal technology
Mental imagery refers to perceptual feel in the absence of sensory input, usually described as seeing with the "mind's optics" or "hearing with the heed's ear" [39]. It is different from perception which occurs when information is directly registered from the senses. Mental imagery is described also every bit the simulation or recreation of perceptual experience across sensory modalities [40]. Pearson [40] has marked ii unlike routes by which mental imagery can exist created within consciousness. Showtime of all, an image tin can exist created directly from firsthand perceptual data. For case, someone tin look at a picture of a horse, create a mental image of the picture in their heed, and so maintain this mental image equally they wait abroad or close their eyes. 2d, an image tin can be created from previously stored information hand in long-term retentiveness. For case, someone tin hear the "horse" and and then create mental imagery based on their previous experience of what a horse expect like.
Imagery has been used frequently in psychotherapy, since the interpretation of dreams by Freud [41]. Today imagination plays a item function in influencing the key characteristics of mental disorders [41]. This aspect is present peculiarly in patients with PTSD which suffer of intrusive imagines, flashback, or sensory memories about their traumatic events [42]. In PTSD, the term flashback is used to describe an intense period of dissociation where patient feels that is reliving a traumatic event [42]. Flashback-blazon mental images have also been identified in other psychological disorders such as social phobia [43], agoraphobia [44], bipolar disorder [45], and also in depression, which is associated with verbal- and imaginative-based procedure, such equally negative rumination. Actually, 90% of depressed patient written report distress intrusive memories of past experiences [46].
Holmes underlines that mental imagery acts every bit an amplifier of emotional furnishings [46]. In fact, imagery has the power to hijack attending (nearly obviously by flashbacks) further away from the external earth, making the internal cognitions more believable and associated emotion more than powerful. Amplified anxiety states consequently affect behavior past the avoidance of anxiety-related triggers, for example, the avoidance of crowded places in agoraphobic anxiety [44]. Other important aspects are that mental imageries are capable to induce learning and to promote behaviors. Thanks to mental exposure and its time to come desensitization, people can face fear situations and acquire positive behaviors [44]. All these characteristics including learning, emotional responses, changing beliefs, and physiological responses could exist translated to VR field. VR can develop simulative environments which are acceptable from the view indicate of sensory bear witness. In fact, VR tin can be considered every bit an advanced imaginal system and an experiential course of imagery that is as effective as reality in inducing cognitive, emotional, and behavioral responses [44]. For that reason, VR exposure therapy has been used in contemporary clinical practice with a strong testify base for treating psychological disorders, such as described previously in this chapter.
There is an increasing evidence that VR exposure is more efficacious than treatment using mental imagery simulations. First of all, the imagination commonly decays quickly. The mental image remains in our mind for approximately 250 ms. [46]. In VR, this risk is not nowadays considering the patient is involved into the environment without the need to evoke whatsoever imagination. Moreover, imagination of previous events needs a good memory and sometimes is not trustful [22]. For instance, during an assessment with PTSD, therapist asks patients to call back nearly a traumatic effect. Sometimes patients fall in this task because memories are not clear. In VR, patients are already involved into traumatic issue, which gives them the possibility to relive the traumatic experience and to face it.
Another important office of VR is to induce positive emotions through positive virtual environments [47]. Information technology is common that relaxing imagination is useful to eliminate stress or negative thoughts from our mind. Thanks to virtual environs, it is possible to involve people into a specific surround to reduce their level of stress (due east.g., virtual island [9]).
To summarize, VR gives an experience that is able to reduce the gap between imagination and reality and to go over retentiveness limits increasing the efficacy and effectiveness of psychotherapy.
3.ii. Embodied applied science
As we have seen, most VR applications take been used to simulate external reality [48]. In fact, in VR it is possible not simply to experience synthetic surround as if it is "our surrounding earth," simply also to experience constructed avatars as if they are "our own body." VR tin be defined also as an "embodied applied science" for "its ability of modifying the feeling of presence" [49]. People'south representations in the virtual earth are usually named avatars, and for the first time in human history, they could permit usa to watch ourselves being others and doing something they accept never washed [49].
Following the betoken, VR as an "embodied applied science" can be useful to change the body'south bounds and to report the human relationship among torso (posture, movements, actions) and noesis and emotions. Moreover, virtual avatars can assist to amplify the "modeling" learning, and therefore to promote the learning of adaptive behaviors.
For instance, literature points out that [fifty] the sense of apotheosis is principally based on 3 main aspects: sense of self-location, sense of agency, and sense of torso buying [50].
Experimental manipulation of the embodied feel is problematic. Even so, the utilize of VR has unique advantages to control the factors associated with the embodied experience. For example, VR makes possible in a relatively like shooting fish in a barrel manner the manipulation of the body representation in terms of structure, morphology, and size, dissociating the egocentric visual perspective from the torso, and exploiting the role of multimodal data in spatiotemporal term for torso perception [52].
For instance, Slater's written report embodied participants alternately in two virtual bodies such that they could accept an extended chat with themselves. In the study, ane body represented themselves and the other represented Dr. Sigmund Freud with whom they would talk over a personal problem. While embodying their own body (lookalike) representation, they described the trouble. They then transfer to the counselor trunk and, from that perspective, saw and heard their lookalike body describing the problem, and so gave some insight into how the problem might be solved. They would then transfer back to their own lookalike trunk and look at and heed to the counselor trunk giving them the advice, and then respond to it. If they chose to, they could and so again see and hear this response from the perspective of the counselor body and again respond to it. This process of switching between the lookalike and counselor body continued until the participant decided to stop. Results showed loftier level of sense of embodiment [52].
Other recent studies have also proved how changing the perspective, and living experiences from other bodies, can assistance the states to promote empathy, and even compassion and self-compassion. For instance, Salter's group has analyzed how the use of virtual bodies can promote compassion and self-compassion. They have analyzed the effects of self-identification with virtual bodies inside immersive VR to increase self-compassion in persons with loftier self-criticism and depression [53]. The same author and his colleagues investigated also how embodied, in VR, a black avatar decreases the racial prejudice [54]. Moreover, Bailenson's grouping has studied how embodied an avatar in VR tin can make u.s.a. better people. For example, participants embodied a Superman avatar and the results evidence that, after the experiment, they felt more helpful [55]. In other Bailenson study, participants embodied a sea coral and, after the experiment, they felt more than sensible to ocean pollution [51].
Other interesting approaches are based on the development of new immersive engineering science named: auto to be another. It is an reward technology to interchange bodies (the real body with the avatar) which offers to the users an immersive feel of seeing themselves in the trunk of another person. MTBA is a low budget body swapping organization, and using a head-mounted display, participant sees the perspective of another person (performer) that mimics his/her movements (Figure two).

Figure 2.
The machine to be another arrangement.
The performer's showtime-person perspective is captured past a camera controlled by user's head movements, revealing torso, legs and arms of the performer's trunk. While interacting with the physical infinite, participants also perceive realistic tactile stimuli. An audio system plays a personal narrative recorded past the performer. The goal of the MTBA is to induce empathy and compassion to participants as the written report of Falconer [53].
To summarize, the potentialities of VR as an "embodied technology" open its use wider than the only reproduction of real worlds. Thank you to this advanced engineering, information technology is possible to study behavioral, cognitive, and emotional aspects that were hard to realize so far. And by designing meaningful embodied activities, VR tin enhance therapy and promote significant changes.
3.three. Connection technology
Recently, software developers and ICT industries accept emphasized that next interesting and compelling piece of work for VR and AR focuses on helping people to connect with others through shared experiences. The new developments of VR are irresolute not only the way people collaborate with computers, simply also the way individuals interact each other. One of the evident signs of this alter has been the creation of totally new interactive communication environments similar estimator-mediated communication (CMC). CMC created a new social space, called cyberspace [56]. Interaction and connection are the key features of internet, from which a sense of self tin can be built. VR, more than other technologies, carries the detachment of interaction from physical interlocutor co-presence to its logical farthermost and challenges the very concept of interlocutor identity. The concept of cyberspace clearly shows that VR is, in fact, a parallel universe created and maintained by the networks in which people interact.
The CMC brought new challenges to clinical psychology. There are objective barriers that stop people the seeking for a therapy program (e.g., geographical distance and lack of local skilled clinicians). To go over all these barriers, new technologies have constitute some solutions. For case, videoconferencing ways simulating face-to-confront psychotherapy using a clinician at a site distant from the client [57]. Some clinicians are not agreeing to utilize videoconference technology for therapy because they argue that the therapeutic alliance volition exist impaired [57]. However, other studies accept shown that therapeutic alliance is established equally well in videoconferencing and face up-to-face therapy and, in some case, participants prefer the online therapy (e.g., younger participants, people living in rural and remote areas). Cybertherapy can go even farther over this problem, thank you to its power to cut geographical limit and to achieve people anywhere and anytime [57]. The growing of new technology gives also the opportunities to interact with people inside the virtual surround. Thank you to this forrard step, it is now possible not just to call a psychotherapist by Skype, but besides to interact with the artificial therapist.
Since several years, virtual surroundings was populated by avatar, a graphical image that represents a person, and it tin interact with real people, thanks to its artificial intelligence (AI). This innovative tool addressed numerous issues in clinical enquiry, cess, and intervention. The first AI tool was "Eliza" that was designed to imitate a Rogerian therapist. The system allowed a computer user to collaborate with a virtual therapist by typing elementary sentence responses to the computerized therapist'southward questions. "Eliza" disappeared soon due its inability to handle complexity questions from the users [58]. A new version of AI therapist was created past the Institute of Creative Applied science, Los Angeles (USA). The plan SimCoach was created to face the urgent need of reducing the stigma of seeking mental health treatment for veteran population who accept a potent PTSD and cutting geographical barriers. SimCoach allows users to initiate and engage in a dialog about their health care concerns with an interactive AI therapist. Mostly, these intelligent graphical characters were designed to employ speech, gestures, and emotions to introduce the capabilities of the organisation, solicit bones anonymous groundwork information most the user'south history and clinical-psychosocial concerns, provide advice and back up, directly the user to relevant online content, and facilitate the process of seeking appropriate care with a live clinical provider. The SimCoach projection is not conceived to deliver a diagnosis or treatment or serve as a replacement for human provides and experts, simply to support users who are determined to be in need, to make the decision to take the first stride toward initiating psychological or medical care with a real psychotherapist, who is the all-time [58].
The connection potential of technology seems to be limitless. Cheers to its feature, it was possible to achieve people who were in demand and without physical or social resource for seeking a therapy assessment.
As we discussed, the three features of VR and AR, imagery, embodiment, and connectedness are primal for the efficacy and effectiveness of cybertherapy. Clinical psychology reached an excellent level in the society, and it contributes to the well-beingness of community. These goals were reached easily, thanks to the supply of new technologies, and in few years, we assist to their potential growth.
Advertisement
4. The future of cybertherapy
The hereafter of VR and AR therapy includes treatment of a wide variety of disorders. Internet dissemination allows therapists piece of cake access to new virtual environments and provides them with a broader selection of options for utilise in therapy. The possibility of offering VR services to patients, nether therapist supervision, at domicile has already become a reality, but this practise has yet to become widespread.
Adding to the previous methods, heady new methods are allowing for the introduction of real digitized images into the virtual globe [22]. This technique was published at the concluding Facebook congress by Mark Zuckerberg. He introduced, in the social virtual world, the possibility to bear witness some personal pictures or the own smartphone pictures to increase the sense of presence [59]. These techniques take the potential to help disorders as attention, social phobia, public speaking, anxiety disorder, PTSD, and then on. For instance, including photograph of child'southward actual classroom, the therapist tin can piece of work with them to improve concentration skills during tests and assignments. In addition, working with the photographs of classmates, co-workers, or family members can assist people to improve their social skills in a safety virtual world and then tin actualize their abilities in the real one [22]. For case, after practicing with the therapist in a closed arrangement, the client can visit a virtual world populated by other avatar, initiate chat, and obtain feedback from other avatars in real time audio.
Another future perspective for the cybertherapy is the use of the "information glove." Information technology allows for tactile interaction in the virtual environment, giving to the users the power to grasp and manipulate virtual objects. This engineering tin be used to increase the sense of presence in the virtual environment, or to help desensitize patients to disturbing tactile stimuli, or to distract them for a painful surgery [22].
As technology advances and more disorders are beingness treated through it, research continues into means in which the boundaries of cybertherapy can be expanded. Engineering science is growing more and more than, and its contribution to clinical psychology will be a crucial issue. Furthermore, in developing new virtual and augmented reality tools, it is important to keep several concepts in heed as therapeutic concept and ethic, the practice and the costs of equipment, and the multidisciplinary teams of experts in item psychologists and engineers.
Ad
5. Determination
A technological revolution in mental wellness intendance is approaching. As Freeman and colleagues take stated, at the forefront may exist virtual and augmented reality, the powerful tools for individuals to make new learning for the benefit of their psychological well-being [60]. Cybertherapy is quickly becoming an accepted and validated method for the handling of many unlike mental disorders. In this chapter, nosotros have described the potential of VR and AR to improve the role of clinic psychology. In Table 2, the advantages and limits of VR and AR in clinical psychology are summarized.
| Advantages | Limits |
|---|---|
| More naturalistic or "real-life" environments | Cost required |
| Command of stimulus presentation and response measurement | Lack of interoperability of VR applications |
| Rubber virtual situations | Dissimilar therapist-patient dynamic |
| Source of information on patient's performance achievements | Basic technological capabilities for therapist and patients |
| Ecological validity | Deficits in sense of presence can influence therapy success |
| Increased standardization of rehabilitation protocols | Cybersickness |
Tabular array two.
Advantages and limits of VR and AR in clinical psychology.
VR and AR have some differences: in VR people are immersed in virtual environments and interact with it. The perception to collaborate with the environment is possible, thank you to the sense of presence (the feeling to be inside the environment); AR is an extension of the real globe, mixing real and bogus reality where people keeping the opportunity to run across their own body, which is not possible with VR, and to interact with the artificial objects. In the concluding decades, many studies accept shown that VR and AR are successful tools for therapy with a high level of efficacy, satisfaction from participants, and subtract in participant's symptoms.
Imagery, embodiment, and connectedness play the keys roles for understanding VR and AR and their potentialities in clinical psychology. In virtual environments, people can experience "as if they are" in a reality that does not be in external globe (imagery applied science). VR/AR also promotes the experience of feeling user's body inside the virtual environment (embodied technology). And now, VR/AR could assist users to connect with others and to share experiences (connectivity engineering). These characteristics have enormous potential for clinical psychology and to ameliorate psychological treatments. However, several barriers yet remain. The first obstacle refers to the expense, especially of designing and creating virtual environments [26]. Nevertheless, the evolution of technologies has reduced the cost dramatically. Now is easy to observe economical equipment and at that place are several free online programs to develop virtual environments. Second, VR software and clinical protocols all the same lack standardization, and most VR systems available are not interoperable. These issues force most researchers to spend a lot of time and money designing and developing "one-off" VR creations. Third, from therapists' side, the performance of PC-based VR programs requires basic calculator skills. In addition, there is a different therapist-patient dynamic in VR therapy that as well must be taken into account. 4th refers to the patient side. The insufficient sense of presence level felt past patients in the virtual environment could negatively affect the therapy. Other barrier from patients is cybersickness, and symptoms can include move sickness, oculomotor problems, and migraines. Ane more barrier regards cultural adaptation. VR applications, every bit other psychological tools, need to be culturally adapted in order to make information technology compatible with the patients' experience and with the general therapeutic goal [12].
Overall, the future of VR and AR seems to be limitless. Technology progress is growing exponentially, and it can generate great and significant changes for clinical psychology. Till now, cybertherapy made huge steps which contributed to the spread of well-being in the lodge, but it is simply on the starting signal. Clinical researchers are working hard to continue the human relationship between clinical psychology and ICTs in privileged position.
Advertizing
Acknowledgments
This chapter was supported past "PROMOSAM" (PSI2014-56303-REDT) and "BODYTA" (Program Nacional I + D + I 2013-2016 PSI2014-51928-R), and Santiago Grisolía programme—Generalitat Valenciana 2017, CIBEROBN is an initiative of the ISCIII (Kingdom of spain).
Advertisement
Disharmonize of interest
There is no financial or personal interest to report.
Advertizement
Abbreviations
| VR | virtual reality |
| AR | augmented reality |
| ICT | information and communication technology |
| PTSD | posttraumatic stress disorder |
| MTBA | car to exist another |
| CMC | computer-mediated communication |
| AI | artificial intelligence |
References
- i.
Riva G, Calvo R, Lisetti C. Cyberpsychology and melancholia computing. In: The Oxford Handbook of Affective Computing. 2015. pp. 547-558. DOI: 10.1093/oxfordhb/9780199942237.013.017 - 2.
Wiederhold MD. Virtual Reality Therapy for Feet Disorders: Advances in Evaluation and Treatment. In: Wiederhold BK, editor. American Periodical of Psychiatry. 2005; 162 (9):1772. DOI:http://dx.doi.org/10.1037/10858-000 - iii.
Botella C, García-Palacios A, Villa H, Baños RM, Quero South, Alcañiz M, et al. Virtual reality exposure in the handling of panic disorder and agoraphobia: A controlled study. Clinical Psychology & Psychotherapy. May ane, 2007; xiv (3):164-175. DOI: 10.1002/cpp.524 - iv.
Baños RM, Guillen V, Quero S, García-Palacios A, Alcaniz One thousand, Botella C. A virtual reality system for the treatment of stress-related disorders: A preliminary analysis of efficacy compared to a standard cognitive behavioral programme. International Journal of Human being-Computer Studies. 2011; 69 (9):602-613. DOI:https://doi.org/ten.1016/j.ijhcs.2011.06.002 - 5.
Botella C, Serrano B, Baños RM, Garcia-Palacios A. Virtual reality exposure-based therapy for the handling of post-traumatic stress disorder: a review of its efficacy, the adequacy of the treatment protocol, and its acceptability. Neuropsychiatric Disease and Handling. Oct iii, 2015; xi :2533-2545. DOI: 10.2147/NDT.S89542 - half-dozen.
Perpiñá C, Botella C, Baños R, Marco H, Alcañiz M, Quero South. Body epitome and virtual reality in eating disorders: Is exposure to virtual reality more constructive than the classical body image handling? CyberPsychology & Beliefs. Apr 1, 1999; 2 (2):149-155. DOI: 10.1089/cpb.1999.2.149 - 7.
Girard B, Turcotte 5, Bouchard S, Girard B. Crushing virtual cigarettes reduces tobacco habit and treatment discontinuation. CyberPsychology & Beliefs. Oct 1, 2009; 12 (v):477-483. DOI: ten.1089/cpb.2009.0118 - 8.
Bordnick PS, Traylor A, Copp HL, Graap KM, Carter B, Ferrer M, et al. Assessing reactivity to virtual reality alcohol based cues. Addictive Behaviors. Jun 1, 2008; 33 (6):743-756. DOI: ten.1016/j.addbeh.2007.12.010 - ix.
Serino S, Cipresso P, Gaggioli A, Pallavicini F, Cipresso Southward, Campanaro D, et al. Smartphone for self-management of psychological stress: a preliminary evaluation of positive applied science app. Revista de Psicopatología y Psicología Clínica. Dec 1, 2014; 19 (three):253-260. DOI: ten.5944/rppc.vol.19.num.iii.2014.13906 - 10.
Baños RM, Espinoza G, García-Palacios A, Cervera JM, Esquerdo G, Barrajón E, et al. A positive psychological intervention using virtual reality for patients with advanced cancer in a hospital setting: A pilot study to assess feasibility. Supportive Care in Cancer. Jan one, 2013; 21 (1):263-270. DOI: 10.1007/s00520-012-1520-x - 11.
Li A, Montaño Z, Chen VJ, Golden JI. Virtual reality and pain management: Current trends and future directions. Pain Direction. Mar 1, 2011; 1 (2):147-157. DOI: ten.2217/pmt.x.15 - 12.
Steuer J. Defining virtual reality: Dimensions determining telepresence. Periodical of Communication. 1992; 42 :73-93. DOI: 10.1111/j.1460-2466.1992.tb00812.ten - 13.
Botella C, Bretón-López J, Quero S, Baños R, García-Palacios A. Treating cockroach phobia with augmented reality. Beliefs Therapy. Sep 1, 2010; 41 (iii):401-413. DOI: 10.1016/j.beth.2009.07.002 - 14.
Alcañiz M, Botella C, Baños RM, Zaragoza I, Guixeres J. The intelligent eastward-therapy system: A new paradigm for telepsychology and cybertherapy. British Journal of Guidance & Counselling. Aug 1, 2009; 37 (3):287-296. DOI: ten.1080/03069880902957015 - xv.
Andersson One thousand. Internet-delivered psychological treatments. Annual Review of Clinical Psychology. 2016; 12 (1):157-179. DOI: x.1146/annurev-clinpsy-021815-093006 - xvi.
Perednia DA, Allen A. Telemedicine engineering science and clinical applications. Journal of the American Medical Association. February 8, 1995; 273 (six):483-488. DOI: 10.1001/jama.1995.03520300057037 - 17.
Chocolate-brown FW. Rural telepsychiatry. Psychiatric Services. Jul ane, 1998; 49 (seven):963-964. DOI: x.1176/ps.49.7.963 - 18.
Eysenbach G and CONSORT-EHEALTH Grouping. Espoused-EHEALTH: Improving and standardizing evaluation reports of web-based and mobile wellness interventions. Journal of Medical Internet Enquiry. Dec 31, 2011; 13 (4):e126. DOI:http://doi.org/10.2196/jmir.1923 - 19.
Alleman JR. Online counseling: The Internet and mental wellness treatment. Psychotherapy: Theory, Research, Practice, Training. 2002; 39 (2):199-209. DOI:http://doi.org/x.2196/jmir.1923 - xx.
Andersson Grand, Titov N. Advantages and limitations of Internet-based interventions for common mental disorders. Globe Psychiatry. 2014; thirteen :iv-11. DOI: 10.1002/wps.20083 - 21.
Mohr DC, Duffecy J, Jin 50, Ludman EJ, Lewis A, Begale Grand, McCarthy Jr M. Multimodal e-mental wellness treatment for depression: A feasibility trial. Journal of Medical Internet Research. Dec nineteen, 2010; 12 (5):e48. DOI:http://doi.org/10.2196/jmir.1370 - 22.
Botella C, Garcia-Palacios A, Baños RM, Quero Due south. Cybertherapy: Advantages, limitations, and upstanding issues. PsychNology Periodical. 2009; 7 (one):77-100 - 23.
Powers MB, Emmelkamp PMG. Virtual reality exposure therapy for anxiety disorders: A meta-assay. Journal of Anxiety Disorders. 2008 April 1; 22 (3):561-569. DOI: 10.1016/j.janxdis.2007.04.006 - 24.
Schultheis MT, Rizzo AA. The application of virtual reality applied science in rehabilitation. Rehabilitation Psychology. 2001; 46 (iii):296-311. DOI: 10.1037/0090-5550.46.3.296 - 25.
Pegden CD. The evolution of simulation languages. In: Advances in Modeling and Simulation [Internet]. Cham: Springer; 2017. pp. 81-96. (Simulation Foundations, Methods and Applications). DOI: 10.1007/978-3-319-64182-9_6 - 26.
Riva G. Virtual reality in psychotherapy: Review. CyberPsychology & Behavior. Jun 1, 2005; 8 (three):220-230. DOI: x.1089/cpb.2005.8.220 - 27.
Jones MC. A laboratory study of fear: The case of peter. The Journal of Genetic Psychology. Dec i, 1991; 152 (four):462-469. DOI: ten.1080/00221325.1991.9914707 - 28.
Sanchez-Vives MV, Slater M. From presence to consciousness through virtual reality. Nature Reviews Neuroscience. Apr 2005; 6 (4):332. DOI: 10.1038/nrn1651 - 29.
Hodges LF, Kooper R, Meyer TC, Rothbaum BO, Opdyke D, de GJJ, et al. Virtual environments for treating the fear of heights. Calculator. Jul 1995; 28 (7):27-34. DOI: 10.1109/ii.391038 - 30.
Opriş D, Pintea Due south, García-Palacios A, Botella C, Szamosközi Ş, David D. Virtual reality exposure therapy in feet disorders: a quantitative meta-assay. Depress Anxiety. 2012; 29 :85-93. DOI: 10.1002/da.20910 - 31.
Botella C, Fernández-Álvarez J, Guillén V, García-Palacios A, Baños R. Recent progress in virtual reality exposure therapy for phobias: A systematic review. Current Psychiatry Reports. Jul 1, 2017; 19 (7):42. DOI: 10.1007/s11920-017-0788-4 - 32.
Botella C, Osma J, Garcia-Palacios A, Quero S, Baños RM. Treatment of flying phobia using virtual reality: data from a 1-yr follow-up using a multiple baseline design. Clinical Psychology & Psychotherapy. 2004; 11 :311-323. DOI: 10.1002/cpp.404 - 33.
Botella C, Baños RM, García-Palacios A, Quero S. Chapter 22 – Virtual Reality and Other Realities A2 – Hofmann, Stefan G. In: Asmundson GJG, editor. The Science of Cognitive Behavioral Therapy [Net]. San Diego: Bookish Press; 2017. pp. 551-590. DOI: 10.1016/B978-0-12-803457-6.00022-2 - 34.
Emmelkamp PM, Krijn One thousand, Hulsbosch A, de Vries S, Schuemie Thou, van der Mast CAP. Virtual reality treatment versus exposure in vivo: a comparative evaluation in acrophobia. Behaviour Research and Therapy. May 1, 2002; 40 (v):509-516. DOI: ten.1016/S0005-7967(01)00023-7 - 35.
Milgram P, Kishino F. A taxonomy of mixed reality visual displays. IEICE Transactions on Information and Systems. December 25, 1994; 77 (12):1321-1329 - 36.
Hughes CE, Stapleton CB, Hughes DE, Smith EM. Mixed reality in instruction, entertainment, and grooming. IEEE Computer Graphics and Applications. November 2005; 25 (6):24-30. DOI: 10.1109/MCG.2005.139 - 37.
Shuhaiber JH. Augmented reality in surgery. Archives of Surgery. February 1, 2004; 139 (ii):170-174. DOI: 10.1001/archsurg.139.two.170 - 38.
Botella C, Perpiñá C, Baños RM, García-Palacios A. Virtual reality: A new clinical setting lab. In: Riva G, Wiederhold BK, Molinari Due east, editors. Studies in Health Technology and Information science, Virtual Environments in Clinical Psychology and Neuroscience: Methods and Techniques in Advanced Patient–Therapist Interaction. Vol. 58. Amsterdam: IOS Press; 1998. pp. 73-81 - 39.
Ji JL, Heyes SB, MacLeod C, Holmes EA. Emotional mental imagery equally simulation of reality: Fear and beyond—A tribute to Peter Lang. Beliefs Therapy. Sep 1, 2016; 47 (five):702-719. DOI: 10.1016/j.beth.2015.eleven.004 - 40.
Pearson DG, Deeprose C, Wallace-Hadrill SMA, Heyes SB, Holmes EA. Assessing mental imagery in clinical psychology: A review of imagery measures and a guiding framework. Clinical Psychology Review. February i, 2013; 33 (1):i-23. DOI: 10.1016/j.cpr.2012.09.001 - 41.
Holmes EA, Bourne C. Inducing and modulating intrusive emotional memories: A review of the trauma film paradigm. Acta Psychologica. Mar 1, 2008; 127 (3):553-566. DOI: 10.1016/j.actpsy.2007.11.002 - 42.
Clark IA, James EL, Iyadurai L, Holmes EA. Mental imagery in psychopathology: From the lab to the clinic. In: Watson LA, Berntsen D, editors. Clinical Perspectives on Autobiographical Retentiveness [Cyberspace]. Cambridge (UK): Cambridge Academy Press; 2015 - 43.
Hackmann A, Clark DM, McManus F. Recurrent images and early on memories in social phobia. Behaviour Enquiry and Therapy. Jun 1, 2000; 38 (6):601-610. DOI: 10.1016/S0005-7967(99)00161-eight - 44.
Day S, Holmes E, Hackmann A. Occurrence of imagery and its link with early on memories in agoraphobia. Retentiveness. Jul i, 2004; 12 (four):416-427. DOI: 10.1080/09658210444000034 - 45.
Holmes EA, Geddes JR, Colom F, Goodwin GM. Mental imagery as an emotional amplifier: Application to bipolar disorder. Behaviour Research and Therapy. December 1, 2008; 46 (12):1251-1258. DOI: 10.1016/j.brat.2008.09.005 - 46.
Holmes EA, Mathews A. Mental imagery and emotion: A special relationship? Emotion. 2005; v (4):489-497. DOI: x.1037/1528-3542.5.4.489 - 47.
Baños RM, Etchemendy E, Castilla D, García-Palacios A, Quero S, Botella C. Positive mood induction procedures for virtual environments designed for elderly people. Interacting with Computers. May 1, 2012; 24 (iii):131-138. DOI: x.1016/j.intcom.2012.04.002 - 48.
Riva Grand, Baños RM, Botella C, Mantovani F, Gaggioli A. Transforming experience: The potential of augmented reality and virtual reality for enhancing personal and clinical alter. Front Psychiatry. Sep 30, 2016; 7 :164. DOI: ten.3389/fpsyt.2016.00164 - 49.
Longo MR, Schüür F, Kammers MPM, Tsakiris M, Haggard P. What is embodiment? A psychometric approach. Noesis. Jun 1, 2008; 107 (3):978-998. DOI: 10.1016/j.cognition.2007.12.004 - 50.
Kilteni K, Groten R, Slater Thousand. The sense of embodiment in virtual reality. Presence: Teleoperators and Virtual Environments. November ane, 2012; 21 (4):373-387. DOI: 10.1162/PRES_a_00124 - 51.
Fox J, Bailenson JN, Tricase L. The apotheosis of sexualized virtual selves: The Proteus effect and experiences of cocky-objectification via avatars. Computers in Man Behavior. May i, 2013; 29 (three):930-938. DOI: 10.1016/j.chb.2012.12.027 - 52.
Osimo SA, Pizarro R, Spanlang B, Slater M. Conversations between self and cocky as Sigmund Freud—A virtual torso ownership paradigm for cocky-counselling. Scientific Reports. Sep 10, 2015; v :13899. DOI: x.1038/srep13899 - 53.
Falconer CJ, Slater Thou, Rovira A, Male monarch JA, Gilbert P, Antley A, et al. Embodying compassion: A virtual reality prototype for overcoming excessive self-criticism. Plos One. November 12, 2014; 9 (xi):e111933. DOI: 10.1371/journal.pone.0111933 - 54.
Peck TC, Seinfeld S, Aglioti SM, Slater Grand. Putting yourself in the skin of a black avatar reduces implicit racial bias. Consciousness and Cognition. Sep 1, 2013; 22 (3):779-787. DOI: 10.1016/j.concog.2013.04.016 - 55.
Rosenberg RS, Baughman SL, Bailenson JN. Virtual superheroes: Using superpowers in virtual reality to encourage prosocial behavior. Plos 1. Jan 30, 2013; eight (1):e55003. DOI: x.1371/journal.pone.0055003 - 56.
Riva G, Galimberti C. The psychology of internet: A socio-cognitive framework to computer-mediated advice. New Ideas in Psychology. Aug 1, 1997; xv (2):141-158. DOI: 10.1016/S0732-118X(97)00015-9 - 57.
Dunstan DA, Tooth SM. Handling via videoconferencing: A airplane pilot study of commitment by clinical psychology trainees. Australian Periodical of Rural Health. Apr i, 2012; xx (2):88-94. DOI: 10.1111/j.1440-1584.2012.01260.x - 58.
Rizzo A, Lange B, Buckwalter JG, et al. Simcoach: An intelligent virtual man arrangement for providing healthcare data and support. International Journal on Disability and Human Evolution. 2011; 10 (four):277-281. DOI: 10.1515/IJDHD.2011.046 - 59.
Available from: https://www.wired.com/2016/x/oculus-facebook-social-vr/ [Accessed: Jul 10, 2016] - 60.
Freeman D, Reeve S, Robinson A, Ehlers A, Clark D, Spanlang B, et al. Virtual reality in the assessment, understanding, and handling of mental health disorders. Psychological Medicine. Oct 2017; 47 (14):2393-2400. DOI: x.1017/S003329171700040X
Submitted: October 16th, 2017 Reviewed: Jan 24th, 2018 Published: May 23rd, 2018
© 2018 The Writer(s). Licensee IntechOpen. This affiliate is distributed under the terms of the Artistic Eatables Attribution iii.0 License, which permits unrestricted use, distribution, and reproduction in whatsoever medium, provided the original work is properly cited.
spencerthallusithe.blogspot.com
Source: https://www.intechopen.com/chapters/59468
0 Response to "Based on Current Reviews and Meta-analyses We Can Say That Cybertherapy Generally Appears to Work"
Post a Comment